Clinical history:
An 18 year old DSH presented with an ulcerated, 2 cm lump on the point of the chin. Impression smears and fine needle aspirate samples were taken and submitted to the laboratory.
Laboratory testing:
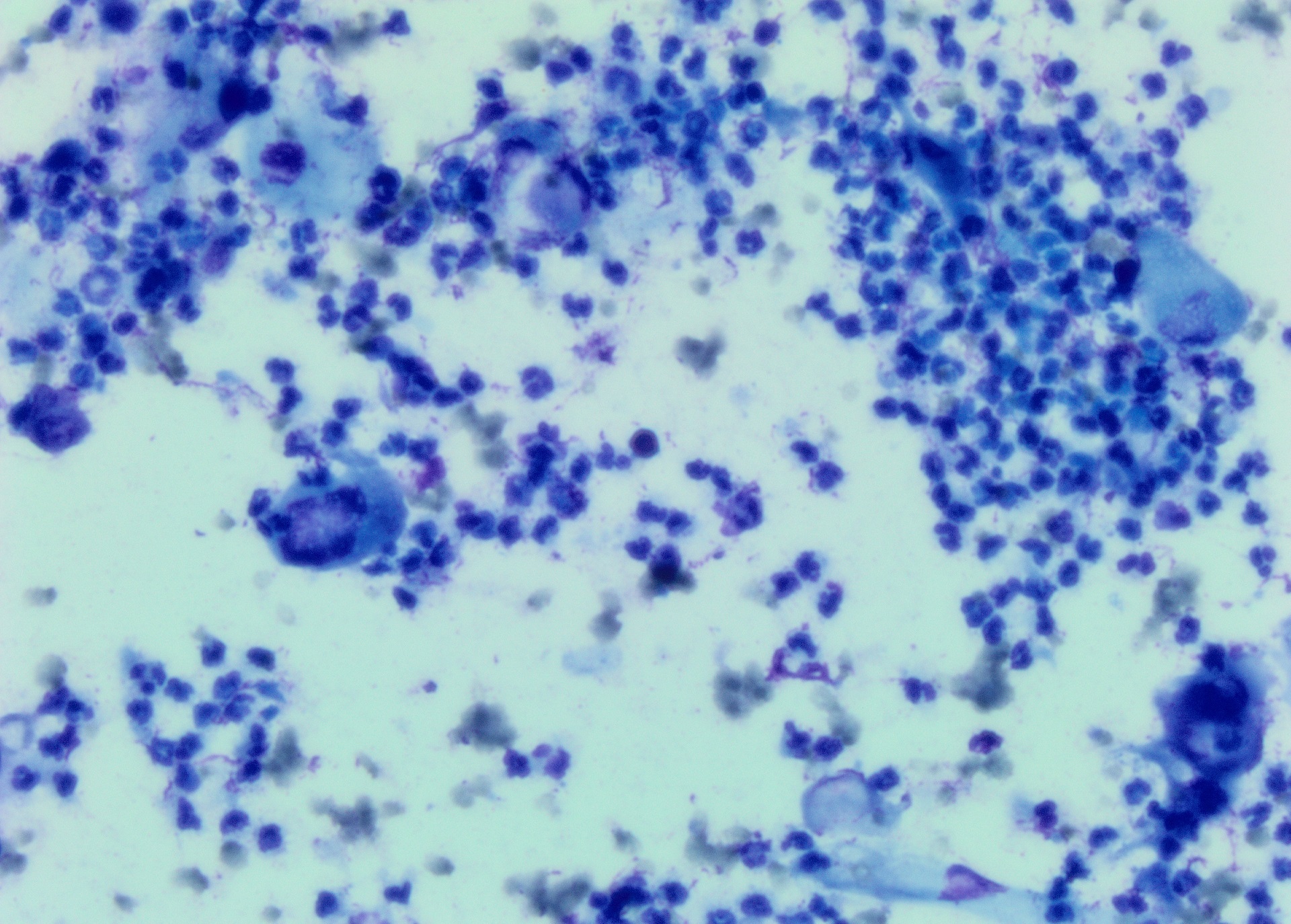
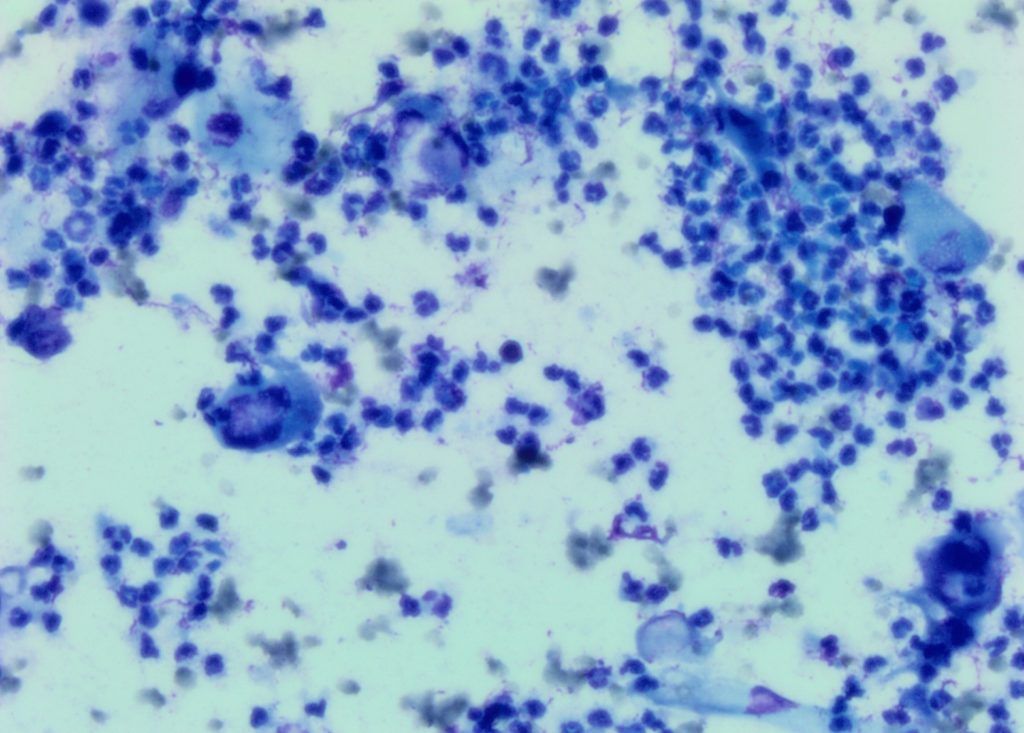
The impression smears were most cellular and the predominant cells, as expected with the ulceration, were inflammatory cells (Figure 1). The cells were mainly neutrophils with low numbers of macrophages. Amongst the inflammatory cells were a significant number of large to very large cells consistent with squamous cells. These cells were elongate to polygonal cells with angular cytoplasmic borders. Most had the blue-green hue to the cytoplasm typical of keratinizing squamous epithelial cells. In many there was asynchrony of nuclear and cytoplasmic maturation, which raised the suspicion that the underlying lesion was a squamous cell carcinoma and the ulceration and suppurative inflammation was secondary. However, there is always the concern that squamous cells can be dysplastic when there is inflammation. An extensive hunt found a few cocci. These were likely secondary from the ulceration.
Figure 1 (right): Impression smear from the ulcerated mass. Large numbers of neutrophils with a few squamous cells. Some of the squamous cells were large with retained nuclei.
Diagnosis:
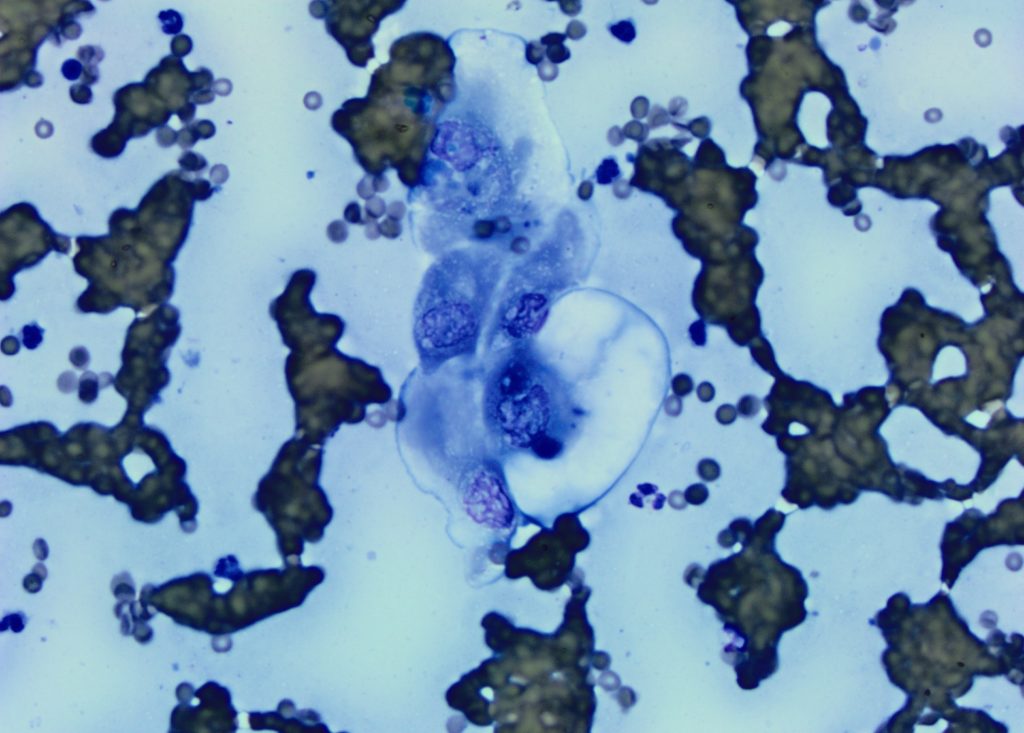
The smears made from aspirates of the mass helped be more certain about the diagnosis of a squamous cell carcinoma. Aspirates from beneath the superficial ulceration yielded quite cellular smears. There were low numbers of neutrophils but the predominant cells were a population of large to very large squamous cells with retained nuclei, cytoplasmic keratinisation and asynchrony of nuclear and cytoplasmic maturation. An example of a cluster of these cells is in Figure 2.
Discussion:
Squamous cell carcinoma is a common tumour in the dog and cat. It accounts for 15% of skin tumours in cats with the face and ears the most common sites. The ulceration and suppurative inflammation which often accompanies these tumours can make it more difficult to be definitive on cytology as dysplastic squamous cells can look atypical. Submitting impression smears plus aspirates from beneath the ulcerated surface is often helpful in being able to make a diagnosis.
MANY THANKS TO EPONA KELLER FROM VETCARE TE RAPA FOR THIS CASE.
Figure 2 (below): A cluster of very large atypical squamous cells found on the smear from the fine needle aspirate.