
KATHRYN JENKINS
We recently had a very rare case of suspected plasma cell leukaemia, with an initial clinical finding of marked hyperglobulinemia.
Clinical history:
After being missing for a week, an 8-year-old cat presented with a jaw mass. In-house biochemistry showed a marked increase in TP (125 g/L; reference interval (RI) 56 – 80 g/L), with a marked hyperglobulinemia (globulin 104 g/L; reference interval 15-57 g/L).
Laboratory results:
A CBC was sent to the laboratory and our Sysmex haematology analyser indicated an abnormal WBC differential scattergram. The WBC count was however within normal limits (16.5 x109/L; reference interval 5.5 – 19.5 x109/L).
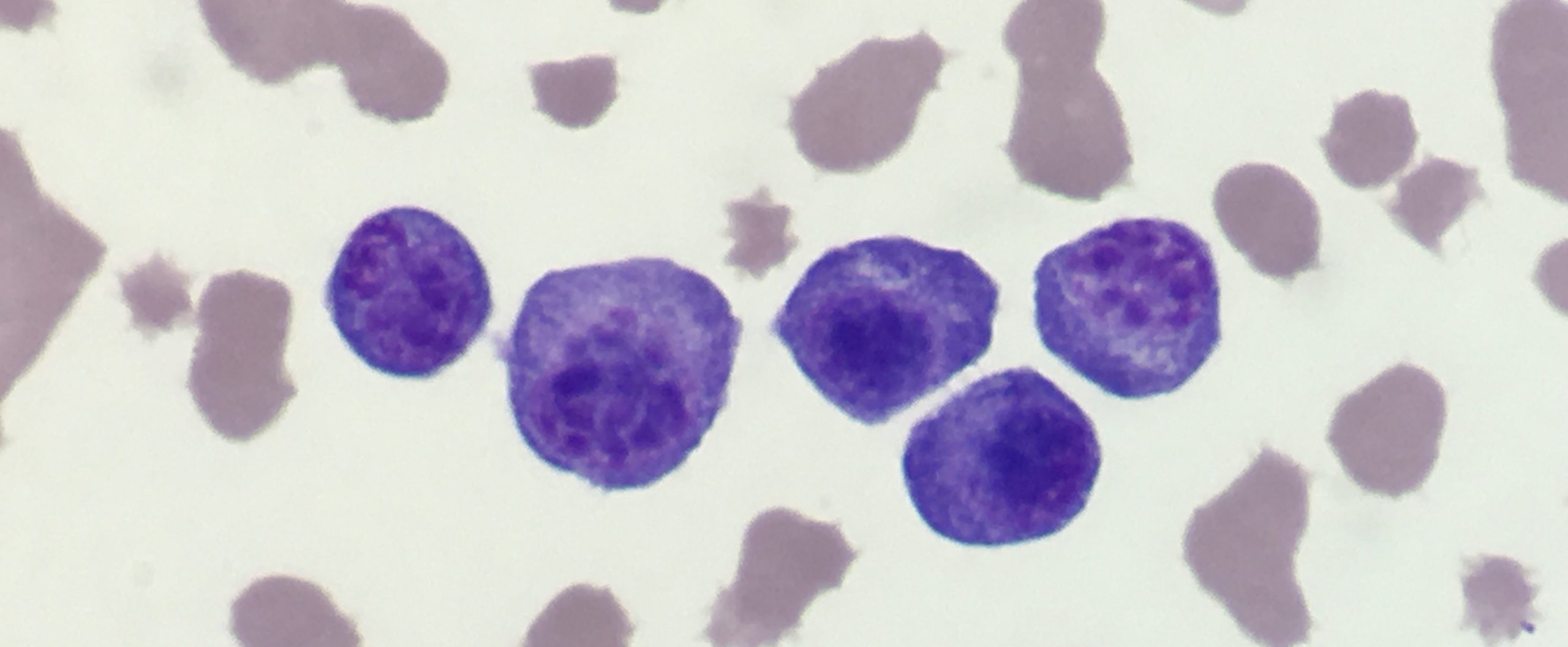
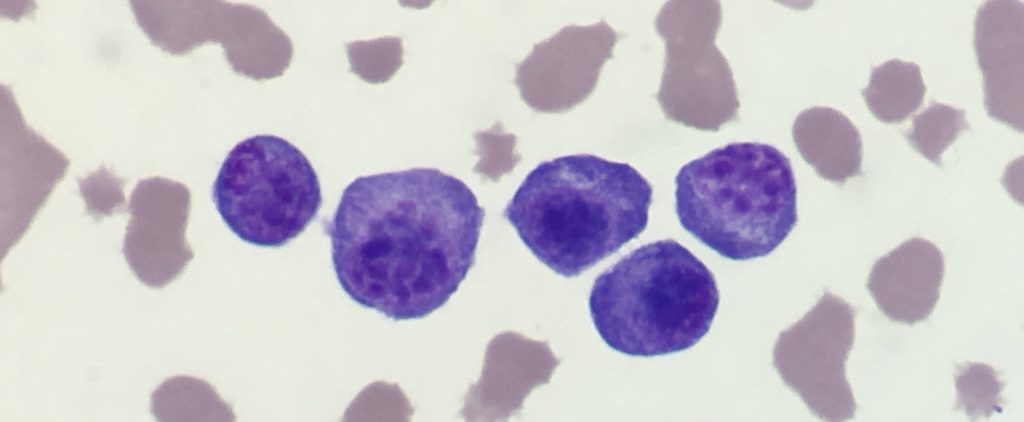
A blood film review demonstrated the presence of many atypical round cells (3.6 x109/L, 22% of all cells). The round cells had features consistent with plasma cells i.e. deeply basophilic cytoplasm, pale perinuclear golgi area and eccentric nuclei with a coarse chromatin pattern (Figure 1).
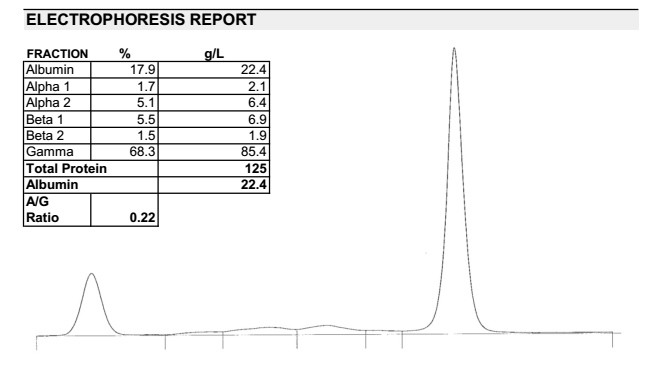
A serum protein electrophoresis tracing (Figure 2) demonstrated a classic monoclonal pattern (tall narrow spike of globulins), which together with the blood film results, supported a neoplastic immunoglobulin secreting B-cell tumour. Although immunophenotyping was not performed, the characteristic morphology of the large number of round cells in circulation was most consistent with plasma cell leukaemia, a rare finding associated with feline myeloma-related disorders. Due to deteriorating condition, and a poor prognosis, the cat was euthanased.
Discussion:
Severe hyperglobulinemia (> 90 g/L in cats) may occur with both chronic inflammatory conditions (such as bacterial pneumonia or FIP), or immunoglobulin secreting B-cell neoplasia (e.g. multiple myeloma, lymphoma). Clinical findings and routine laboratory diagnostics can help elucidate the cause, and serum protein electrophoresis can be used to further differentiate between inflammatory and neoplastic causes of hyperglobulinemia.
Myeloma-related disorder (MRD) is an umbrella term, encompassing several diagnostic categories of immunoglobulin secreting B-cell neoplasia. This includes cutaneous plasmacytoma, multiple myeloma and non-cutaneous extramedullary plasma cell neoplasia, as well as various leukaemias, lymphoma and solitary plasmacytoma of bone.
In contrast to both dogs and humans when it comes to infiltrative plasma cell neoplasia, in cats extramedullary involvement of neoplastic plasma cell infiltration is a common finding. There can be a wide spectrum of dissemination – with the spleen, liver and lymph nodes most frequently involved. A non-regenerative anaemia and hypocholesterolemia are common concurrent findings. Variable degrees of bone marrow infiltration with neoplastic plasma cells can be demonstrated in some cases, however true multiple myeloma (with characteristic radiographically detectable bone lesions) appears to be a less common presentation in cats.
Similar to their canine counterparts, cases of feline cutaneous plasmacytoma appear benign in behaviour and can respond well to surgical excision. However unlike dogs, there is a greater potential for underlying multi-organ involvement and paraproteinaemia in cats with cutaneous plasma cell tumours.
In both cats and dogs, circulating neoplastic plasma cells are rarely seen, and only a handful of plasma cell leukaemia cases have been reported in veterinary medicine. Human literature defines plasma cell leukaemia as having an abnormal number of myeloma cells in peripheral circulation (>2 x109/L or > 20% plasmacytosis), with supportive paraproteinaemia and immunophenotyping (e.g. MUM1+, Pax5-). Plasma cell leukaemia has a poor prognosis, with reported cases displaying aggressive behaviour.
Thank you to Dr Magdeline Soo, of Cahill Animal Hospital for this interesting case.
References:
· Mellor, P.J. et al. Histopathologic, Immunohistochemical, and Cytologic Analysis of Feline Myeloma-Related Disorders: Further Evidence for Primary Extramedullary Development in the Cat. Vet. Pathol. 45:159-173, 2008.
· Takeuchi, Y. et al. Myeloma-related disorder with leukaemic progression in a cat. J. Feline Med. Surg. 12:982-7, 2010.