
Sandra Bulla
Clinical history
A 10-year-old male, neutered domestic cat presented at his local veterinarian with multiple dermal/subcutaneous nodules. The nodules were moderately firm and were present all over the trunk in variable sizes, with the larger nodule being 3cm wide. They were not painful, and the cat was well otherwise. Fine needle biopsy was taken from one of the nodules and sent to our laboratory for cytology.
Cytology findings
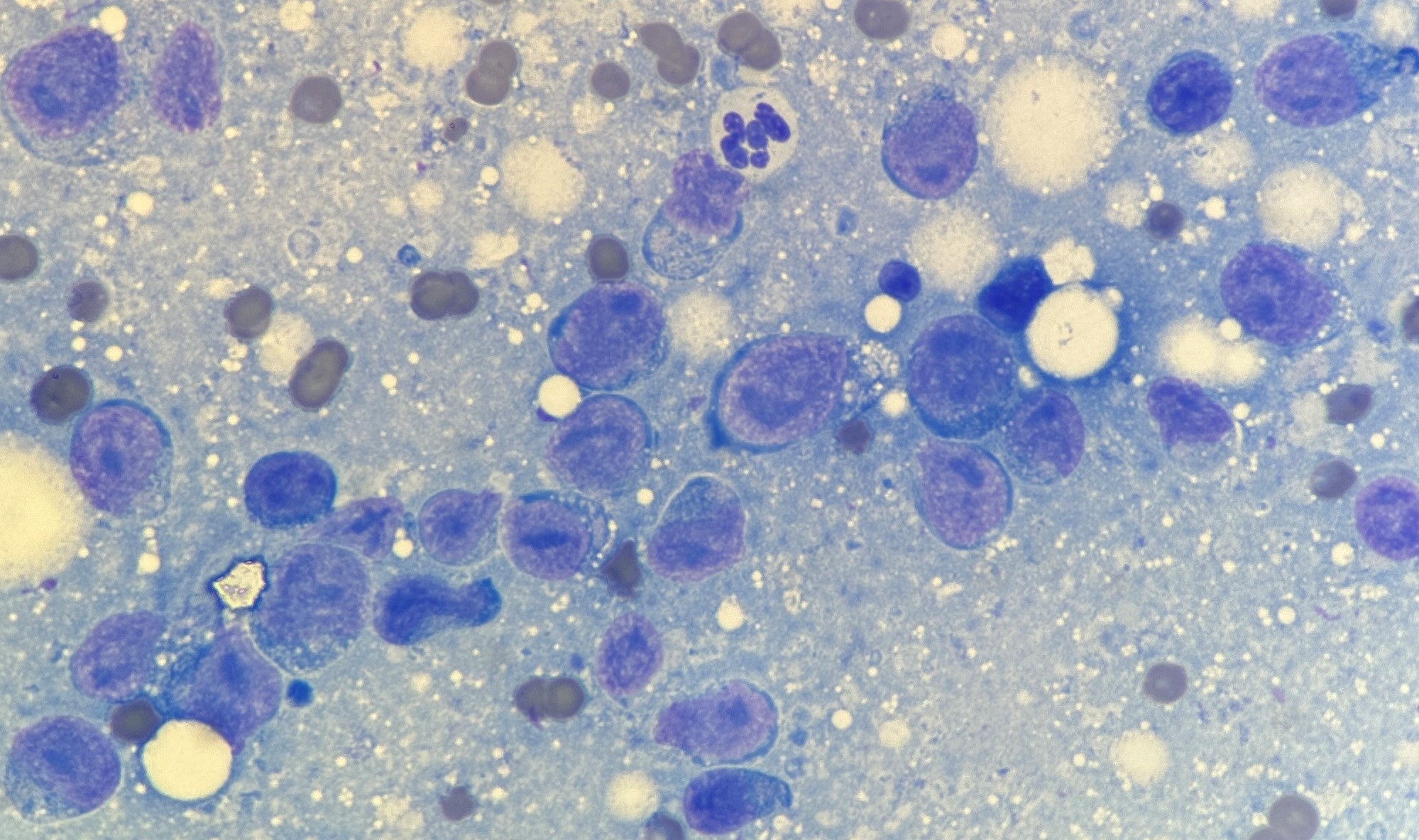
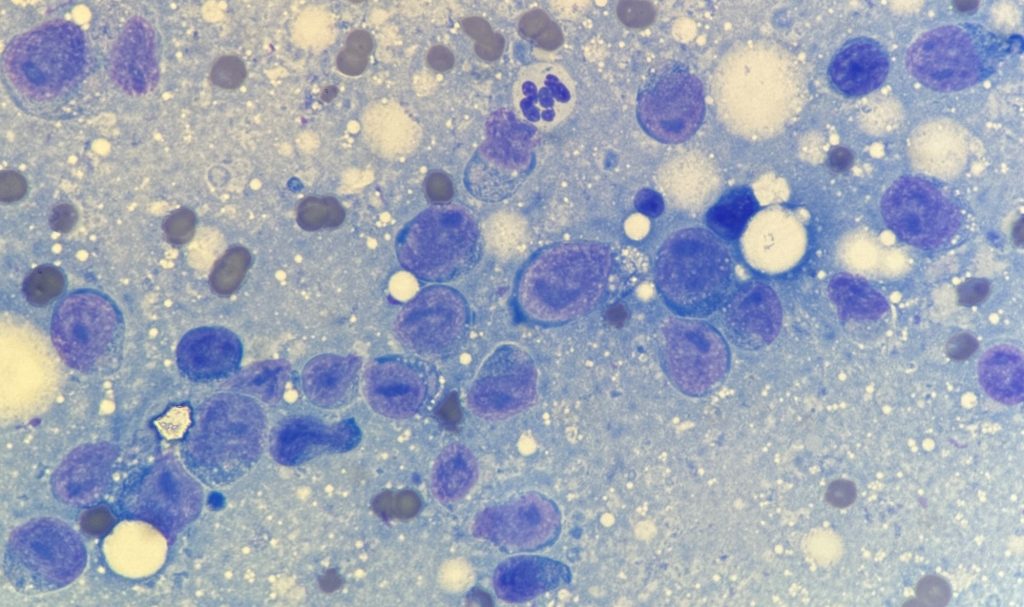
Examination of the slides revealed a homogenous population of large lymphocytes. These cells had small amounts of dark basophilic cytoplasm and a round nucleus with multiple large prominent nucleoli (Figure 1). The cytologic diagnosis was large cell lymphoma.
Discussion
Although both lymphoma and skin neoplasia are very common occurrences in cats, cutaneous lymphoma is rare. Due to the paucity of cases reported, little is known about this disease. Patients present with various clinical signs, including itching, alopecia, scaly skin, skin redness, loss of skin colour, ulcers, nodules, pustules, and plaques. The distribution of skin changes can be highly variable, and patients can have a multifocal disease distribution. Lesions are most reported on the limbs, trunk and head, and any patients present with varying types of lesions (Siewert et al., 2022).
As seen in dogs and humans, cutaneous lymphomas in cats are classified in two forms, depending on the distribution of the neoplastic lymphocytes in the skin.
The epitheliotropic form, which is characterized by neoplastic cells exhibiting tropism for the epidermis with secondary extension into the dermis, is less common in cats. The cell of origin of this type of neoplasia is most often T-cells, and it can be further classified as mycosis fungoides or pagetoid reticulosis on histopathology.
The non-epitheliotropic cutaneous lymphoma affects the dermis and subcutis without involvement of the epidermis and can be either of T-cell or B-cell origin. This is the more common condition in cats and can be subclassified as indolent T-cell lymphoma (or cutaneous lymphocytosis), diffuse T-cell lymphoma, T-cell-rich large B-cell lymphoma, and lymphoplasmacytic lymphoma (Roccabianca et al., 2016).
Although both epitheliotropic and non-epitheliotropic forms often have a similar clinical appearance, some presentations are more commonly seen in one of the subtypes of feline cutaneous lymphoma. The epitheliotropic form often presents lesions that include exfoliative erythroderma, patches, plaques, erosions and ulcers, lesions at mucocutaneous junctions and in the oral cavity. The non-epitheliotropic lymphoma usually presents as non-pruritic solitary or multifocal plaques and/or nodules that are often ulcerated. These lesions can occasionally have erythema, crusting and scaling.
Despite the differences seen between the two forms and the subtypes, immunophenotype, cell size, and the presence of epitheliotropism was not found to be associated with response to treatment (Siewert et al., 2022).
Cutaneous lymphoma is mostly seen in older cats with no apparent breed or sex predispositions. Prognosis is grave, with median survival time of 6-12 months.
Aetiology is still poorly understood in feline cutaneous lymphoma. For more common lymphomas there is an evident association with viruses (feline leukaemia virus and feline immunodeficiency virus), but such a relationship has not been established for the cutaneous form. However, it appears that the occurrence of cutaneous lymphoma can be related with inflammatory reactions in cats. There are reports of cutaneous lymphomas developing at injection sites and this specific presentation of cutaneous lymphoma shared some clinical and pathological features with feline injection site sarcomas and with lymphomas developing in the setting of subacute to chronic inflammation reported in human beings (Roccabianca et al., 2016). Another interesting distinct presentation was a cutaneous non-epitheliotropic T-cell lymphoma that developed at the site of a previous traumatic bone fracture and metal orthopaedic implant (Jegatheeson et al., 2018).
Additionally, there is a specific form of cutaneous lymphoma that originates near or around the tarsal joint and clinically appears as a subcutaneous mass. The reason for this location is still uncertain. Although further investigation is required to better characterise this disease, most of these cases appeared to be non-epitheliotropic, of high grade, and of B-cell phenotype (Burr et al., 2014).
In conclusion, feline cutaneous lymphoma is a rare but aggressive disease. Considering that the skin changes often seen can be similar to numerous non-neoplastic conditions, including parasitic or infectious diseases; and allergic disorders, such as eosinophilic granuloma complex, it should always be a differential diagnosis for any swelling, nodule, lesion or mass within the dermis or subcutis, regardless of bodily location. Given this ability to mimic benign skin diseases, it is possible that proper diagnosis and treatment is often delayed, which may contribute to the poor prognosis in these patients. This reinforces the value of the collection of fine needle biopsies from skin lesions on older cats once they first present at the veterinary clinic. Lymphoma is very often easily diagnosed on cytology, which will allow a prompt initiation of a therapy protocol if needed.
References
> Burr HD, Keating JH, Clifford CA, Burgess KE. Cutaneous lymphoma of the tarsus in cats: 23 cases (2000–2012). J Am Vet Med Assoc. 244:1429-1434, 2014.
> Jegatheeson S, Wayne J, Brockley LK. Cutaneous non-epitheliotropic T-cell lymphoma associated with a fracture site in a cat. JFMS Open Rep. 2018 Mar 9;4(1): 2055116918760357.
> Roccabianca P, Avallone G, Rodriguez A, et al. Cutaneous Lymphoma at Injection Sites: Pathological, Immunophenotypical, and Molecular Characterization in 17 Cats. Vet Pathol. 53:823-832, 2016.
> Siewert J, Pellin MA, Husbands BD, Curran KM, Scavelli D, Sampene E. Feline cutaneous lymphoma: an evaluation of disease presentation and factors affecting response to treatment. J Feline Med Surg. 24:389-397, 2022.